 Thai
Thai

What Is an Inverted Nipple?
An inverted nipple is a condition in which the nipple does not protrude outward but is instead pulled inward, making it not visible in the normal way. It can be present from birth or develop later in life, may affect one or both sides, and can occur in both women and men.
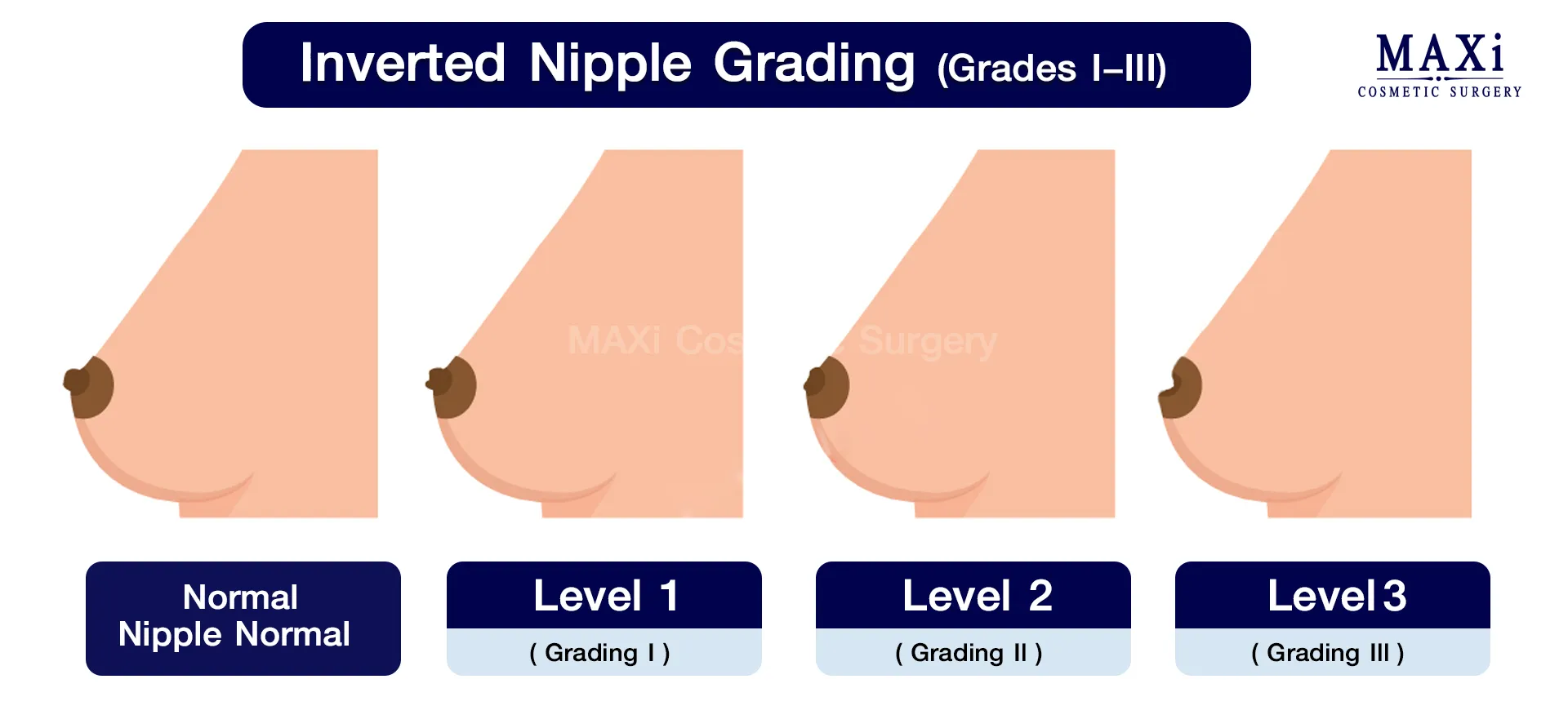
Grading of Inverted Nipples (Grade I–III)
The most widely referenced classification system is Han & Hong (1999), which divides inverted nipples into three grades to guide treatment planning:
Grade I: The nipple can be pulled out manually or stimulated to protrude, and it stays out temporarily. Grade II: The nipple can be pulled out but retracts back within a short time. Grade III: The nipple cannot be pulled out at all due to shortened milk ducts or tightly constricting fibrous tissue.
Does an Inverted Nipple Affect Health?
While an inverted nipple is not classified as a serious medical condition, it can have several impacts:
1. Impact on Breastfeeding A nipple that does not protrude can make it difficult for an infant to latch, making feeding uncomfortable. In severe cases (Grade III), the milk ducts may be too shortened or restricted, making breastfeeding very difficult.
2. Hygiene and Infection Risk A deeply retracted nipple tends to trap moisture and debris, increasing the risk of irritation, inflammation, or unpleasant odor. Some individuals may develop mastitis (breast inflammation) if hygiene is not maintained properly.
3. A Warning Sign for Breast Conditions In people whose nipples were previously normal but later became inverted, this may be a warning sign of a breast-related condition or abnormal breast tissue. A doctor should be consulted promptly.
Inverted Nipples and Self–Confidence
Medically, inverted nipples may not pose a serious threat, but psychologically they can have a significant impact — particularly for women, since the nipple is a defining feature of the breast’s appearance.
- Men with inverted nipples may feel self-conscious about removing their shirt.
- Some individuals have concerns about their appearance in intimate relationships.
- Inverted nipples are therefore often considered an aesthetic issue that many people wish to correct for the sake of confidence.
Who Is a Good Candidate — and Who Is Not?
Suitable for:
- Those whose inverted nipples cause problems with breastfeeding, skin irritation, moisture buildup, recurring infections, or affect their self-confidence.
- Those who understand the limitations regarding recurrence risk and impact on breastfeeding, and have made a well-considered decision.
Not suitable for:
- Pregnant or breastfeeding individuals (it is advisable to wait until hormones and milk ducts have stabilized).
- Those with active breast inflammation or infection (the infection must be treated first).

Treatment Options
1. Non–Surgical Methods — Suitable for Grade I, but results may not be permanent:
- Nipple massage and stimulation
- Nipple shields or vacuum suction devices
2. Surgical Correction For Grades I–III, surgical correction is the most effective permanent solution. The surgeon releases the fibrous tissue or milk ducts that are pulling the nipple inward.
Surgical Techniques
1. Duct–Sparing Technique
- Suitable for Grades I–III
- Releases constricting fibrous tissue/fibers and sutures the nipple base to hold it in place
- Advantage: Better potential for future breastfeeding; smaller incision
- Note: Slightly higher recurrence rate in some cases compared to duct-cutting
2. Duct–Cutting / Division Technique
- Typically used for Grade III or severe recurrent cases
- The constricting ducts/fibrous tissue are cut and tissue is added to support the nipple
- Advantage: Reduces the chance of the nipple retracting again
- Note: Often affects future breastfeeding ability

Can I Breastfeed After Surgery?
- Duct–sparing technique: There is a greater chance of being able to breastfeed afterward (though not guaranteed).
- Duct–cutting technique: This usually affects breastfeeding ability.
It is important to clearly communicate your plans regarding pregnancy and breastfeeding from the outset so the surgeon can recommend the most appropriate technique.
How Long Is the Recovery?
With MAXi Clinic’s technique, patients can return to daily activities immediately after surgery without taking time off work. Just 1 day after the procedure, the wound can safely get wet.
Pre–Operative Preparation
- Inform your doctor if you are pregnant, breastfeeding, or planning to have children.
- Stop certain medications or supplements as advised.
- Quit smoking (to reduce the risk of slow wound healing, infection, and certain inflammatory conditions associated with smoking).
Post–Operative Care at MAXi Clinic
First 24–72 Hours:
- Apply cold compresses and send photos to monitor your condition as instructed.
- Avoid pressure or friction on the nipple, especially when sleeping face-down.
- Wear a well-fitting bra — not too tight.
Weeks 1–2:
- Attend follow-up appointments; keep the wound dry and clean.
- Avoid swimming and saunas; avoid activities that involve chest impact or heavy arm swinging.
Risks and Possible Complications
- Hematoma, bruising, swelling, and pain
- Wound infection
- Numbness or abnormal nipple sensitivity
- Loss of breastfeeding ability (more common with duct-cutting techniques)
- Recurrence requiring repeat surgery (risk varies by technique and individual)